You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
"WW C"- COVID-19, GLOBAL CASES SURPASS 676 MILLION...CASES 676,609,955 DEATHS 6,881,955 US CASES 103,804,263 US DEATHS 1,123,836 8:30pm 1/28/24
- Thread starter lightbright
- Start date
-
- Tags
- vaccination


Mask dispute at Vancouver gym leaves one man beaten and bloody
Victim was allegedly punched and pushed, hitting his head on exercise equipment after falling during the incident.

5 confirmed COVID-19 cases at Vancouver Police Department, dozens of members self-isolating
Five Vancouver police employees have recently tested positive for COVID-19 at three different locations, prompting another 27 sworn and civilian members to self-isolate as a result.
bc.ctvnews.ca

COVID-19 emergency benefits including CRB, sickness benefit, to be extended: Trudeau - National | Globalnews.ca
Prime Minister Justin Trudeau says emergency COVID-19 benefits are getting a top-up, as the pandemic continues to rage across the country.
 globalnews.ca
globalnews.ca

Anti-masker berates employees at camera store in Vancouver (VIDEO) | News
The employees at Kerrisdale Cameras in Vancouver were harrassed after an anti-masker entered the store and tried to make a purchase last week.
 dailyhive.com
dailyhive.com

As antimaskers plan "freedom rally", ICBC reveals that just five percent of provincial COVID-19 fines have been paid
Most of the fines imposed under the federal Quarantine Act in B.C. also haven't been paid.
 www.straight.com
www.straight.com

Two women ‘dressed up as grannies’ tried to get vaccinated in Florida
The women, aged 34 and 44, presented valid CDC cards indicating that they had already received their first coronavirus vaccine doses, said the health administrator for Orange County. “I don’t know how they escaped the first time,” he said.
The women, aged 34 and 44, presented valid CDC cards indicating that they had already received their first coronavirus vaccine doses, said the health administrator for Orange County. “I don’t know how they escaped the first time,” he said.
Japan Discovers New Coronavirus Variant
The variant, which the country’s health department said appears to have originated overseas, has infected nearly 100 people.
 A medical worker fills a syringe with a dose of the Pfizer-BioNTech COVID-19 vaccine, Feb. 17, 2021, in Tokyo.
A medical worker fills a syringe with a dose of the Pfizer-BioNTech COVID-19 vaccine, Feb. 17, 2021, in Tokyo.
JAPAN ON FRIDAY confirmed a new coronavirus variant that has infected nearly 100 people.
Reuters reported that Chief Cabinet Secretary Katsunobu Kato told reporters that 91 infections were documented in the Kanto area of eastern Japan and two other cases were discovered at airports.
"It may be more contagious than conventional strains, and if it continues to spread domestically, it could lead to a rapid rise in cases," Kato said.
The variant has a mutation on the spike protein that could lower the efficacy of vaccines.
The National Institute of Infectious Diseases said that the variant appears to have originated overseas, but it is different from other variants circulating in Britain, South Africa and Brazil.
Japan has over 422,000 cases of the virus and 7,360 deaths, according to data from Johns Hopkins University.
The country's health ministry reports Japan has reported 150 cases of the other variants first found in Britain, South Africa and Brazilian travelers.
The variants have complicated the outbreak's outlook, with speculation that the highly infectious strain first documented in the U.K. could become the dominant one in the U.S. in March.
Experts have said it is now a race to get as many people vaccinated as possible to help control the spread of the variants.
Japan Discovers New Coronavirus Variant | Health News | US News
The variant, which the country’s health department said appears to have originated overseas, has infected nearly 100 people.
JAPAN ON FRIDAY confirmed a new coronavirus variant that has infected nearly 100 people.
Reuters reported that Chief Cabinet Secretary Katsunobu Kato told reporters that 91 infections were documented in the Kanto area of eastern Japan and two other cases were discovered at airports.
"It may be more contagious than conventional strains, and if it continues to spread domestically, it could lead to a rapid rise in cases," Kato said.
The variant has a mutation on the spike protein that could lower the efficacy of vaccines.
The National Institute of Infectious Diseases said that the variant appears to have originated overseas, but it is different from other variants circulating in Britain, South Africa and Brazil.
Japan has over 422,000 cases of the virus and 7,360 deaths, according to data from Johns Hopkins University.
The country's health ministry reports Japan has reported 150 cases of the other variants first found in Britain, South Africa and Brazilian travelers.
The variants have complicated the outbreak's outlook, with speculation that the highly infectious strain first documented in the U.K. could become the dominant one in the U.S. in March.
Experts have said it is now a race to get as many people vaccinated as possible to help control the spread of the variants.
Japan Discovers New Coronavirus Variant | Health News | US News
Should You Get the COVID-19 Vaccine if You Have Sickle Cell Anemia?
Meg Burke, MD
Meg Burke, MD, is a board-certified physician and medical writer. She is a practicing primary care geriatrician.
February 4, 2021, 1:55PM (PT)
Key takeaways:
Infection with COVID-19 is a new and serious threat for people with sickle cell anemia. The virus can take advantage of the weakened immune systems of people with the disease and cause devastating harm.
Luckily, there are steps that at-risk people can take to minimize their risk of infection with COVID-19. Medical advances, including vaccines and new treatment protocols, are bringing hope that we can provide more protection to people with sickle cell anemia (and other high-risk conditions) while there is still ongoing community spread of the virus.
This piece addresses the unique challenges that individuals with sickle cell anemia are facing during this pandemic and why they should prioritize getting the COVID-19 vaccine.
What is sickle cell anemia?
Sickle cell anemia (also called sickle cell disease) is a disorder of red blood cells. People are born with sickle cell anemia (you cannot catch it).
Red blood cells carry oxygen from your lungs to the rest of your body. In sickle cell anemia, the red blood cells are a different shape and size than normal red blood cells, which can lead to serious issues. With even a small problem (like not drinking enough water or getting a minor infection), people who have sickle cell anemia can feel very sick. They may require hospitalization for treatment and pain control. They can also develop complications like acute chest syndrome, which can be deadly.
Who is most likely to be diagnosed with sickle cell anemia?
Almost 100,000 people in the United States have sickle cell anemia. Most of the people diagnosed are Black or African American. About 1 in every 365 Black or African American babies born in the United States has sickle cell anemia.
Don't miss out on savings!
Get the best ways to save on your prescriptions delivered to your inbox.
By signing up, I agree to GoodRx's terms of service and privacy policy, and to receive marketing messages from GoodRx.
Are people with sickle cell anemia at a higher risk for severe COVID-19?
Yes, they are. People with sickle cell anemia who have COVID-19 infection are more likely to be hospitalized and to require intensive level care (ICU) in the hospital. They are also more likely to die from COVID-19 than people without sickle cell anemia.
One study followed 178 people with sickle cell anemia and COVID-19 infection. The average age of people in the study was less than 40 years old. Sixty-nine percent of people needed to be treated in a hospital, and 7% of them died.
Is the COVID-19 vaccine safe for people with sickle cell anemia?
Yes, the COVID-19 vaccine is safe for people with sickle cell disease.
All routine vaccines for adults and children are recommended for people with sickle cell anemia. There are studies that show that two common vaccines, the pneumococcal and influenza (“flu”) vaccines, are effective in people with sickle cell anemia. People with sickle cell anemia should be prioritized as a high-risk group to receive the yearly influenza vaccine.
There are many similarities between the COVID-19 vaccines and other vaccines that work for people with sickle cell anemia. So there is no reason to think that the COVID-19 vaccines would not be safe or effective in people with sickle cell anemia. In fact, the Centers for Disease Control and Prevention (CDC) has recommended that people with sickle cell disease be prioritized to receive the vaccine (more on this later).
How does the COVID-19 vaccine work?
The two FDA-approved COVID-19 vaccines, Pfizer/BioNTech and Moderna, work by giving your cells “directions” for how to make a small piece of protein that belongs to the COVID-19 virus. Once the small piece of protein is made, your immune system (the system in your body that fights infections) recognizes this protein as something it has never seen before.
This kicks your immune system into gear to start making tools (“antibodies”) to fight off the virus. It makes a small number of antibodies after the first dose of the vaccine, and even more antibodies after the second vaccine because it is better prepared to respond to the protein.
Then, when and if you are exposed to the COVID-19 virus, your body already has the tools to fight it off and prevent you from developing symptoms and serious illness from the actual virus.
Are people with sickle cell disease considered high priority for COVID-19 vaccination?
The CDC recognizes sickle cell anemia as a condition that puts people at high risk for serious illness from COVID-19. They recommend that adults 16 to 64 years old with sickle cell anemia receive the vaccine in Phase 1c. This is after Phase 1a (healthcare providers and long-term care residents) and Phase 1b (people ≥75 years old and essential workers who are not healthcare providers). Currently in the United States, each state is deciding their priority groups for giving out the vaccine on their own.
Can the COVID-19 vaccine interact with any medications for sickle cell disease?
We don’t know the answer to this question. We do know that the most common medication used to treat sickle cell anemia, hydroxyurea, does not affect the immune response that comes from other commonly used vaccines. People on other medications that treat sickle cell anemia, such as voxelotor and crizanlizumab, should discuss their unique situation and the COVID-19 vaccine with their healthcare provider.
Other considerations for people with sickle cell disease
There are two groups of people with sickle cell disease who either are not able to receive the vaccine or must wait before they take it.
Under age 16
The current COVID-19 vaccines are not approved for anyone under age 16, including people with sickle cell anemia. There are currently active trials looking to see how safe the vaccines are and how well they work in people younger than 16 years old. Vaccine recommendations will be reconsidered once the vaccines are approved for this group.
Already had COVID-19
The approved vaccines are safe to give to people who have already had COVID-19 infection. But people who have received certain treatments, including monoclonal antibodies or convalescent plasma, should wait at least 90 days from the last day of treatment to receive the COVID-19 vaccine. This is to prevent the treatment that they received from making the vaccine less effective.
How can people with sickle cell anemia protect themselves against COVID-19 until vaccination is possible?
People with sickle cell anemia should follow all CDC guidelines to protect themselves against COVID-19 infection before they receive the vaccine. The three most important guidelines are below:
People with sickle cell anemia are at increased risk for serious COVID-19 infections. We have safe and effective vaccines that protect against COVID-19 infection. People over age 16 with sickle cell anemia should prioritize receiving their COVID-19 vaccine when it is available to them.
.
Meg Burke, MD
Meg Burke, MD, is a board-certified physician and medical writer. She is a practicing primary care geriatrician.
February 4, 2021, 1:55PM (PT)
Key takeaways:
- Sickle cell anemia can put you at increased risk of serious complications from COVID-19.
- All routine vaccines are safe, effective, and strongly recommended for people with sickle cell anemia.
- Adults and children over 16 years old with sickle cell anemia should get the COVID-19 vaccine.
Infection with COVID-19 is a new and serious threat for people with sickle cell anemia. The virus can take advantage of the weakened immune systems of people with the disease and cause devastating harm.
Luckily, there are steps that at-risk people can take to minimize their risk of infection with COVID-19. Medical advances, including vaccines and new treatment protocols, are bringing hope that we can provide more protection to people with sickle cell anemia (and other high-risk conditions) while there is still ongoing community spread of the virus.
This piece addresses the unique challenges that individuals with sickle cell anemia are facing during this pandemic and why they should prioritize getting the COVID-19 vaccine.
What is sickle cell anemia?
Sickle cell anemia (also called sickle cell disease) is a disorder of red blood cells. People are born with sickle cell anemia (you cannot catch it).
Red blood cells carry oxygen from your lungs to the rest of your body. In sickle cell anemia, the red blood cells are a different shape and size than normal red blood cells, which can lead to serious issues. With even a small problem (like not drinking enough water or getting a minor infection), people who have sickle cell anemia can feel very sick. They may require hospitalization for treatment and pain control. They can also develop complications like acute chest syndrome, which can be deadly.
Who is most likely to be diagnosed with sickle cell anemia?
Almost 100,000 people in the United States have sickle cell anemia. Most of the people diagnosed are Black or African American. About 1 in every 365 Black or African American babies born in the United States has sickle cell anemia.
Don't miss out on savings!
Get the best ways to save on your prescriptions delivered to your inbox.
By signing up, I agree to GoodRx's terms of service and privacy policy, and to receive marketing messages from GoodRx.
Are people with sickle cell anemia at a higher risk for severe COVID-19?
Yes, they are. People with sickle cell anemia who have COVID-19 infection are more likely to be hospitalized and to require intensive level care (ICU) in the hospital. They are also more likely to die from COVID-19 than people without sickle cell anemia.
One study followed 178 people with sickle cell anemia and COVID-19 infection. The average age of people in the study was less than 40 years old. Sixty-nine percent of people needed to be treated in a hospital, and 7% of them died.
Is the COVID-19 vaccine safe for people with sickle cell anemia?
Yes, the COVID-19 vaccine is safe for people with sickle cell disease.
All routine vaccines for adults and children are recommended for people with sickle cell anemia. There are studies that show that two common vaccines, the pneumococcal and influenza (“flu”) vaccines, are effective in people with sickle cell anemia. People with sickle cell anemia should be prioritized as a high-risk group to receive the yearly influenza vaccine.
There are many similarities between the COVID-19 vaccines and other vaccines that work for people with sickle cell anemia. So there is no reason to think that the COVID-19 vaccines would not be safe or effective in people with sickle cell anemia. In fact, the Centers for Disease Control and Prevention (CDC) has recommended that people with sickle cell disease be prioritized to receive the vaccine (more on this later).
How does the COVID-19 vaccine work?
The two FDA-approved COVID-19 vaccines, Pfizer/BioNTech and Moderna, work by giving your cells “directions” for how to make a small piece of protein that belongs to the COVID-19 virus. Once the small piece of protein is made, your immune system (the system in your body that fights infections) recognizes this protein as something it has never seen before.
This kicks your immune system into gear to start making tools (“antibodies”) to fight off the virus. It makes a small number of antibodies after the first dose of the vaccine, and even more antibodies after the second vaccine because it is better prepared to respond to the protein.
Then, when and if you are exposed to the COVID-19 virus, your body already has the tools to fight it off and prevent you from developing symptoms and serious illness from the actual virus.
Are people with sickle cell disease considered high priority for COVID-19 vaccination?
The CDC recognizes sickle cell anemia as a condition that puts people at high risk for serious illness from COVID-19. They recommend that adults 16 to 64 years old with sickle cell anemia receive the vaccine in Phase 1c. This is after Phase 1a (healthcare providers and long-term care residents) and Phase 1b (people ≥75 years old and essential workers who are not healthcare providers). Currently in the United States, each state is deciding their priority groups for giving out the vaccine on their own.
Can the COVID-19 vaccine interact with any medications for sickle cell disease?
We don’t know the answer to this question. We do know that the most common medication used to treat sickle cell anemia, hydroxyurea, does not affect the immune response that comes from other commonly used vaccines. People on other medications that treat sickle cell anemia, such as voxelotor and crizanlizumab, should discuss their unique situation and the COVID-19 vaccine with their healthcare provider.
Other considerations for people with sickle cell disease
There are two groups of people with sickle cell disease who either are not able to receive the vaccine or must wait before they take it.
Under age 16
The current COVID-19 vaccines are not approved for anyone under age 16, including people with sickle cell anemia. There are currently active trials looking to see how safe the vaccines are and how well they work in people younger than 16 years old. Vaccine recommendations will be reconsidered once the vaccines are approved for this group.
Already had COVID-19
The approved vaccines are safe to give to people who have already had COVID-19 infection. But people who have received certain treatments, including monoclonal antibodies or convalescent plasma, should wait at least 90 days from the last day of treatment to receive the COVID-19 vaccine. This is to prevent the treatment that they received from making the vaccine less effective.
How can people with sickle cell anemia protect themselves against COVID-19 until vaccination is possible?
People with sickle cell anemia should follow all CDC guidelines to protect themselves against COVID-19 infection before they receive the vaccine. The three most important guidelines are below:
- Wear a mask that covers your mouth and nose when you are around anyone outside of your household.
- Stay distanced from other people, even when you are wearing a mask. The closest that you should get to other people is 6 feet, but farther away is better.
- Avoid any crowded spaces or unnecessary travel.
People with sickle cell anemia are at increased risk for serious COVID-19 infections. We have safe and effective vaccines that protect against COVID-19 infection. People over age 16 with sickle cell anemia should prioritize receiving their COVID-19 vaccine when it is available to them.
.
We’ll Have Herd Immunity by April
Covid cases have dropped 77% in six weeks. Experts should level with the public about the good news.
Amid the dire Covid warnings, one crucial fact has been largely ignored: Cases are down 77% over the past six weeks. If a medication slashed cases by 77%, we’d call it a miracle pill. Why is the number of cases plummeting much faster than experts predicted?
In large part because natural immunity from prior infection is far more common than can be measured by testing. Testing has been capturing only from 10% to 25% of infections, depending on when during the pandemic someone got the virus. Applying a time-weighted case capture average of 1 in 6.5 to the cumulative 28 million confirmed cases would mean about 55% of Americans have natural immunity.
Now add people getting vaccinated. As of this week, 15% of Americans have received the vaccine, and the figure is rising fast. Former Food and Drug Commissioner Scott Gottlieb estimates 250 million doses will have been delivered to some 150 million people by the end of March.
There is reason to think the country is racing toward an extremely low level of infection. As more people have been infected, most of whom have mild or no symptoms, there are fewer Americans left to be infected. At the current trajectory, I expect Covid will be mostly gone by April, allowing Americans to resume normal life.
Antibody studies almost certainly underestimate natural immunity. Antibody testing doesn’t capture antigen-specific T-cells, which develop “memory” once they are activated by the virus. Survivors of the 1918 Spanish flu were found in 2008—90 years later—to
have memory cells still able to produce neutralizing antibodies.
Researchers at Sweden’s Karolinska Institute found that the percentage of people mounting a T-cell response after mild or asymptomatic Covid-19 infection consistently exceeded the percentage with detectable antibodies. T-cell immunity was even present in people who were exposed to infected family members but never developed symptoms. A group of U.K. scientists in September pointed out that the medical community may be under-appreciating the prevalence of immunity from activated T-cells.
Covid-19 deaths in the U.S. would also suggest much broader immunity than recognized. About 1 in 600 Americans has died of Covid-19, which translates to a population fatality rate of about 0.15%. The Covid-19 infection fatality rate is about 0.23%. These numbers indicate that roughly two-thirds of the U.S. population has had the infection.
In my own conversations with medical experts, I have noticed that they too often dismiss natural immunity, arguing that we don’t have data. The data certainly doesn’t fit the classic randomized-controlled-trial model of the old-guard medical establishment. There’s no control group. But the observational data is compelling.
I have argued for months that we could save more American lives if those with prior Covid-19 infection forgo vaccines until all vulnerable seniors get their first dose. Several studies demonstrate that natural immunity should protect those who had Covid-19 until more vaccines are available. Half my friends in the medical community told me: Good idea. The other half said there isn’t enough data on natural immunity, despite the fact that reinfections have occurred in less than 1% of people—and when they do occur, the cases are mild.
But the consistent and rapid decline in daily cases since Jan. 8 can be explained only by natural immunity. Behavior didn’t suddenly improve over the holidays; Americans traveled more over Christmas than they had since March. Vaccines also don’t explain the steep decline in January. Vaccination rates were low and they take weeks to kick in.
My prediction that Covid-19 will be mostly gone by April is based on laboratory data, mathematical data, published literature and conversations with experts. But it’s also based on direct observation of how hard testing has been to get, especially for the poor. If you live in a wealthy community where worried people are vigilant about getting tested, you might think that most infections are captured by testing. But if you have seen the many barriers to testing for low-income Americans, you might think that very few infections have been captured at testing centers. Keep in mind that most infections are asymptomatic, which still triggers natural immunity.
Many experts, along with politicians and journalists, are afraid to talk about herd immunity. The term has political overtones because some suggested the U.S. simply let Covid rip to achieve herd immunity. That was a reckless idea. But herd immunity is the inevitable result of viral spread and vaccination. When the chain of virus transmission has been broken in multiple places, it’s harder for it to spread—and that includes the new strains.
Herd immunity has been well-documented in the Brazilian city of Manaus, where researchers in the Lancet reported the prevalence of prior Covid-19 infection to be 76%, resulting in a significant slowing of the infection. Doctors are watching a new strain that threatens to evade prior immunity. But countries where new variants have emerged, such as the U.K., South Africa and Brazil, are also seeing significant declines in daily new cases. The risk of new variants mutating around the prior vaccinated or natural immunity should be a reminder that Covid-19 will persist for decades after the pandemic is over. It should also instill a sense of urgency to develop, authorize and administer a vaccine targeted to new variants.
Some medical experts privately agreed with my prediction that there may be very little Covid-19 by April but suggested that I not to talk publicly about herd immunity because people might become complacent and fail to take precautions or might decline the vaccine. But scientists shouldn’t try to manipulate the public by hiding the truth. As we encourage everyone to get a vaccine, we also need to reopen schools and society to limit the damage of closures and prolonged isolation. Contingency planning for an open economy by April can deliver hope to those in despair and to those who have made large personal sacrifices.
We’ll Have Herd Immunity by April - WSJ
Covid cases have dropped 77% in six weeks. Experts should level with the public about the good news.
Amid the dire Covid warnings, one crucial fact has been largely ignored: Cases are down 77% over the past six weeks. If a medication slashed cases by 77%, we’d call it a miracle pill. Why is the number of cases plummeting much faster than experts predicted?
In large part because natural immunity from prior infection is far more common than can be measured by testing. Testing has been capturing only from 10% to 25% of infections, depending on when during the pandemic someone got the virus. Applying a time-weighted case capture average of 1 in 6.5 to the cumulative 28 million confirmed cases would mean about 55% of Americans have natural immunity.
Now add people getting vaccinated. As of this week, 15% of Americans have received the vaccine, and the figure is rising fast. Former Food and Drug Commissioner Scott Gottlieb estimates 250 million doses will have been delivered to some 150 million people by the end of March.
There is reason to think the country is racing toward an extremely low level of infection. As more people have been infected, most of whom have mild or no symptoms, there are fewer Americans left to be infected. At the current trajectory, I expect Covid will be mostly gone by April, allowing Americans to resume normal life.
Antibody studies almost certainly underestimate natural immunity. Antibody testing doesn’t capture antigen-specific T-cells, which develop “memory” once they are activated by the virus. Survivors of the 1918 Spanish flu were found in 2008—90 years later—to
have memory cells still able to produce neutralizing antibodies.
Researchers at Sweden’s Karolinska Institute found that the percentage of people mounting a T-cell response after mild or asymptomatic Covid-19 infection consistently exceeded the percentage with detectable antibodies. T-cell immunity was even present in people who were exposed to infected family members but never developed symptoms. A group of U.K. scientists in September pointed out that the medical community may be under-appreciating the prevalence of immunity from activated T-cells.
Covid-19 deaths in the U.S. would also suggest much broader immunity than recognized. About 1 in 600 Americans has died of Covid-19, which translates to a population fatality rate of about 0.15%. The Covid-19 infection fatality rate is about 0.23%. These numbers indicate that roughly two-thirds of the U.S. population has had the infection.
In my own conversations with medical experts, I have noticed that they too often dismiss natural immunity, arguing that we don’t have data. The data certainly doesn’t fit the classic randomized-controlled-trial model of the old-guard medical establishment. There’s no control group. But the observational data is compelling.
I have argued for months that we could save more American lives if those with prior Covid-19 infection forgo vaccines until all vulnerable seniors get their first dose. Several studies demonstrate that natural immunity should protect those who had Covid-19 until more vaccines are available. Half my friends in the medical community told me: Good idea. The other half said there isn’t enough data on natural immunity, despite the fact that reinfections have occurred in less than 1% of people—and when they do occur, the cases are mild.
But the consistent and rapid decline in daily cases since Jan. 8 can be explained only by natural immunity. Behavior didn’t suddenly improve over the holidays; Americans traveled more over Christmas than they had since March. Vaccines also don’t explain the steep decline in January. Vaccination rates were low and they take weeks to kick in.
My prediction that Covid-19 will be mostly gone by April is based on laboratory data, mathematical data, published literature and conversations with experts. But it’s also based on direct observation of how hard testing has been to get, especially for the poor. If you live in a wealthy community where worried people are vigilant about getting tested, you might think that most infections are captured by testing. But if you have seen the many barriers to testing for low-income Americans, you might think that very few infections have been captured at testing centers. Keep in mind that most infections are asymptomatic, which still triggers natural immunity.
Many experts, along with politicians and journalists, are afraid to talk about herd immunity. The term has political overtones because some suggested the U.S. simply let Covid rip to achieve herd immunity. That was a reckless idea. But herd immunity is the inevitable result of viral spread and vaccination. When the chain of virus transmission has been broken in multiple places, it’s harder for it to spread—and that includes the new strains.
Herd immunity has been well-documented in the Brazilian city of Manaus, where researchers in the Lancet reported the prevalence of prior Covid-19 infection to be 76%, resulting in a significant slowing of the infection. Doctors are watching a new strain that threatens to evade prior immunity. But countries where new variants have emerged, such as the U.K., South Africa and Brazil, are also seeing significant declines in daily new cases. The risk of new variants mutating around the prior vaccinated or natural immunity should be a reminder that Covid-19 will persist for decades after the pandemic is over. It should also instill a sense of urgency to develop, authorize and administer a vaccine targeted to new variants.
Some medical experts privately agreed with my prediction that there may be very little Covid-19 by April but suggested that I not to talk publicly about herd immunity because people might become complacent and fail to take precautions or might decline the vaccine. But scientists shouldn’t try to manipulate the public by hiding the truth. As we encourage everyone to get a vaccine, we also need to reopen schools and society to limit the damage of closures and prolonged isolation. Contingency planning for an open economy by April can deliver hope to those in despair and to those who have made large personal sacrifices.
We’ll Have Herd Immunity by April - WSJ
One of my favorite rappers is a dummy
I am not too sure about this especially with the different variants out thereWe’ll Have Herd Immunity by April
Covid cases have dropped 77% in six weeks. Experts should level with the public about the good news.
Amid the dire Covid warnings, one crucial fact has been largely ignored: Cases are down 77% over the past six weeks. If a medication slashed cases by 77%, we’d call it a miracle pill. Why is the number of cases plummeting much faster than experts predicted?
In large part because natural immunity from prior infection is far more common than can be measured by testing. Testing has been capturing only from 10% to 25% of infections, depending on when during the pandemic someone got the virus. Applying a time-weighted case capture average of 1 in 6.5 to the cumulative 28 million confirmed cases would mean about 55% of Americans have natural immunity.
Now add people getting vaccinated. As of this week, 15% of Americans have received the vaccine, and the figure is rising fast. Former Food and Drug Commissioner Scott Gottlieb estimates 250 million doses will have been delivered to some 150 million people by the end of March.
There is reason to think the country is racing toward an extremely low level of infection. As more people have been infected, most of whom have mild or no symptoms, there are fewer Americans left to be infected. At the current trajectory, I expect Covid will be mostly gone by April, allowing Americans to resume normal life.
Antibody studies almost certainly underestimate natural immunity. Antibody testing doesn’t capture antigen-specific T-cells, which develop “memory” once they are activated by the virus. Survivors of the 1918 Spanish flu were found in 2008—90 years later—to
have memory cells still able to produce neutralizing antibodies.
Researchers at Sweden’s Karolinska Institute found that the percentage of people mounting a T-cell response after mild or asymptomatic Covid-19 infection consistently exceeded the percentage with detectable antibodies. T-cell immunity was even present in people who were exposed to infected family members but never developed symptoms. A group of U.K. scientists in September pointed out that the medical community may be under-appreciating the prevalence of immunity from activated T-cells.
Covid-19 deaths in the U.S. would also suggest much broader immunity than recognized. About 1 in 600 Americans has died of Covid-19, which translates to a population fatality rate of about 0.15%. The Covid-19 infection fatality rate is about 0.23%. These numbers indicate that roughly two-thirds of the U.S. population has had the infection.
In my own conversations with medical experts, I have noticed that they too often dismiss natural immunity, arguing that we don’t have data. The data certainly doesn’t fit the classic randomized-controlled-trial model of the old-guard medical establishment. There’s no control group. But the observational data is compelling.
I have argued for months that we could save more American lives if those with prior Covid-19 infection forgo vaccines until all vulnerable seniors get their first dose. Several studies demonstrate that natural immunity should protect those who had Covid-19 until more vaccines are available. Half my friends in the medical community told me: Good idea. The other half said there isn’t enough data on natural immunity, despite the fact that reinfections have occurred in less than 1% of people—and when they do occur, the cases are mild.
But the consistent and rapid decline in daily cases since Jan. 8 can be explained only by natural immunity. Behavior didn’t suddenly improve over the holidays; Americans traveled more over Christmas than they had since March. Vaccines also don’t explain the steep decline in January. Vaccination rates were low and they take weeks to kick in.
My prediction that Covid-19 will be mostly gone by April is based on laboratory data, mathematical data, published literature and conversations with experts. But it’s also based on direct observation of how hard testing has been to get, especially for the poor. If you live in a wealthy community where worried people are vigilant about getting tested, you might think that most infections are captured by testing. But if you have seen the many barriers to testing for low-income Americans, you might think that very few infections have been captured at testing centers. Keep in mind that most infections are asymptomatic, which still triggers natural immunity.
Many experts, along with politicians and journalists, are afraid to talk about herd immunity. The term has political overtones because some suggested the U.S. simply let Covid rip to achieve herd immunity. That was a reckless idea. But herd immunity is the inevitable result of viral spread and vaccination. When the chain of virus transmission has been broken in multiple places, it’s harder for it to spread—and that includes the new strains.
Herd immunity has been well-documented in the Brazilian city of Manaus, where researchers in the Lancet reported the prevalence of prior Covid-19 infection to be 76%, resulting in a significant slowing of the infection. Doctors are watching a new strain that threatens to evade prior immunity. But countries where new variants have emerged, such as the U.K., South Africa and Brazil, are also seeing significant declines in daily new cases. The risk of new variants mutating around the prior vaccinated or natural immunity should be a reminder that Covid-19 will persist for decades after the pandemic is over. It should also instill a sense of urgency to develop, authorize and administer a vaccine targeted to new variants.
Some medical experts privately agreed with my prediction that there may be very little Covid-19 by April but suggested that I not to talk publicly about herd immunity because people might become complacent and fail to take precautions or might decline the vaccine. But scientists shouldn’t try to manipulate the public by hiding the truth. As we encourage everyone to get a vaccine, we also need to reopen schools and society to limit the damage of closures and prolonged isolation. Contingency planning for an open economy by April can deliver hope to those in despair and to those who have made large personal sacrifices.
We’ll Have Herd Immunity by April - WSJ
I am not too sure about this especially with the different variants out there
You're also not an epidemiologist or virology so there's that.

The problem is that the public, especially the US population, has already demonstrated that they are collectively dense. If people start talking about herd immunity being a lock by April, people will definitely nut up and do stupid shit until then, and probably make things worse.We’ll Have Herd Immunity by April
Covid cases have dropped 77% in six weeks. Experts should level with the public about the good news.
Amid the dire Covid warnings, one crucial fact has been largely ignored: Cases are down 77% over the past six weeks. If a medication slashed cases by 77%, we’d call it a miracle pill. Why is the number of cases plummeting much faster than experts predicted?
In large part because natural immunity from prior infection is far more common than can be measured by testing. Testing has been capturing only from 10% to 25% of infections, depending on when during the pandemic someone got the virus. Applying a time-weighted case capture average of 1 in 6.5 to the cumulative 28 million confirmed cases would mean about 55% of Americans have natural immunity.
Now add people getting vaccinated. As of this week, 15% of Americans have received the vaccine, and the figure is rising fast. Former Food and Drug Commissioner Scott Gottlieb estimates 250 million doses will have been delivered to some 150 million people by the end of March.
There is reason to think the country is racing toward an extremely low level of infection. As more people have been infected, most of whom have mild or no symptoms, there are fewer Americans left to be infected. At the current trajectory, I expect Covid will be mostly gone by April, allowing Americans to resume normal life.
Antibody studies almost certainly underestimate natural immunity. Antibody testing doesn’t capture antigen-specific T-cells, which develop “memory” once they are activated by the virus. Survivors of the 1918 Spanish flu were found in 2008—90 years later—to
have memory cells still able to produce neutralizing antibodies.
Researchers at Sweden’s Karolinska Institute found that the percentage of people mounting a T-cell response after mild or asymptomatic Covid-19 infection consistently exceeded the percentage with detectable antibodies. T-cell immunity was even present in people who were exposed to infected family members but never developed symptoms. A group of U.K. scientists in September pointed out that the medical community may be under-appreciating the prevalence of immunity from activated T-cells.
Covid-19 deaths in the U.S. would also suggest much broader immunity than recognized. About 1 in 600 Americans has died of Covid-19, which translates to a population fatality rate of about 0.15%. The Covid-19 infection fatality rate is about 0.23%. These numbers indicate that roughly two-thirds of the U.S. population has had the infection.
In my own conversations with medical experts, I have noticed that they too often dismiss natural immunity, arguing that we don’t have data. The data certainly doesn’t fit the classic randomized-controlled-trial model of the old-guard medical establishment. There’s no control group. But the observational data is compelling.
I have argued for months that we could save more American lives if those with prior Covid-19 infection forgo vaccines until all vulnerable seniors get their first dose. Several studies demonstrate that natural immunity should protect those who had Covid-19 until more vaccines are available. Half my friends in the medical community told me: Good idea. The other half said there isn’t enough data on natural immunity, despite the fact that reinfections have occurred in less than 1% of people—and when they do occur, the cases are mild.
But the consistent and rapid decline in daily cases since Jan. 8 can be explained only by natural immunity. Behavior didn’t suddenly improve over the holidays; Americans traveled more over Christmas than they had since March. Vaccines also don’t explain the steep decline in January. Vaccination rates were low and they take weeks to kick in.
My prediction that Covid-19 will be mostly gone by April is based on laboratory data, mathematical data, published literature and conversations with experts. But it’s also based on direct observation of how hard testing has been to get, especially for the poor. If you live in a wealthy community where worried people are vigilant about getting tested, you might think that most infections are captured by testing. But if you have seen the many barriers to testing for low-income Americans, you might think that very few infections have been captured at testing centers. Keep in mind that most infections are asymptomatic, which still triggers natural immunity.
Many experts, along with politicians and journalists, are afraid to talk about herd immunity. The term has political overtones because some suggested the U.S. simply let Covid rip to achieve herd immunity. That was a reckless idea. But herd immunity is the inevitable result of viral spread and vaccination. When the chain of virus transmission has been broken in multiple places, it’s harder for it to spread—and that includes the new strains.
Herd immunity has been well-documented in the Brazilian city of Manaus, where researchers in the Lancet reported the prevalence of prior Covid-19 infection to be 76%, resulting in a significant slowing of the infection. Doctors are watching a new strain that threatens to evade prior immunity. But countries where new variants have emerged, such as the U.K., South Africa and Brazil, are also seeing significant declines in daily new cases. The risk of new variants mutating around the prior vaccinated or natural immunity should be a reminder that Covid-19 will persist for decades after the pandemic is over. It should also instill a sense of urgency to develop, authorize and administer a vaccine targeted to new variants.
Some medical experts privately agreed with my prediction that there may be very little Covid-19 by April but suggested that I not to talk publicly about herd immunity because people might become complacent and fail to take precautions or might decline the vaccine. But scientists shouldn’t try to manipulate the public by hiding the truth. As we encourage everyone to get a vaccine, we also need to reopen schools and society to limit the damage of closures and prolonged isolation. Contingency planning for an open economy by April can deliver hope to those in despair and to those who have made large personal sacrifices.
We’ll Have Herd Immunity by April - WSJ
If we can get through the "first wave" cases (because we never really had a wave end here), we might be able to manage the variants without a crazy amount of outbreaks. But the ignorance train is getting worse each day.
He is the most negative person.You're also not an epidemiologist or virology so there's that.
I agree we have too many variance out there to have heard Immunity. Plus a good chunk of American people are just stupidThe problem is that the public, especially the US population, has already demonstrated that they are collectively dense. If people start talking about herd immunity being a lock by April, people will definitely nut up and do stupid shit until then, and probably make things worse.
If we can get through the "first wave" cases (because we never really had a wave end here), we might be able to manage the variants without a crazy amount of outbreaks. But the ignorance train is getting worse each day.

Trivia night at Port Moody pub considered a COVID-19 super-spreader| CityNews Vancouver
The event at St. James's Well has prompted action from WorkSafeBC. An industry group insists COVID-19 spread would have been prevented if customers followed the rules.
 www.citynews1130.com
www.citynews1130.com
More optimistic news. . .

 www.latimes.com
www.latimes.com
New optimism that COVID-19 is finally dwindling as L.A. gains some herd immunity
In L.A., so many people now have immunity to the coronavirus from past infections and vaccination that transmission is slowing and inching toward herd immunity.
www.latimes.com
Someone sent me this video. It has a lot of information for and about us.
Outstanding! Thank you for this! I’m following up on everything he said. I’m still going to get the vaccine if offered. Man there was some hard hitting info in this! The Doc is pro black too and a soldier!
Probably hid their results to not look like jackasses.I bet none of those vampires tested positive for it huh?
One reason why Biden is doing better because he is allowing his scientist to come out and educate the public
Someone sent me this video. It has a lot of information for and about us.
Good post... Be following Dr. Rolling for a minute
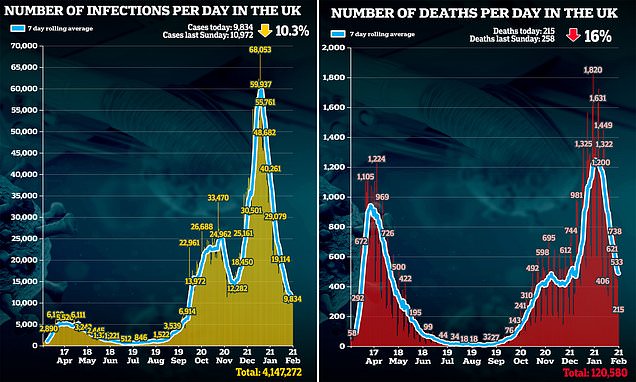
UK records 9,834 more Covid cases - down 10% on last week
Covid-19 infection rates have continued to drop with 9,834 more coronavirus cases - a fall of 10 per cent on last week - while the 215 new daily deaths brought Britain's total up to 120,580.

Crowds flock to parks and beauty spots on hottest day of the year
Crowds of people broke lockdown rules and flocked to tourist spots across the UK yesterday as they enjoyed sunning themselves during the hottest day of 2021 so far as temperatures hit 60F.

COVID Deaths Pass 500,000 in U.S.
More Americans have died from COVID than on the battlefield in WWI, II & 'Nam combined.
 www.tmz.com
www.tmz.com

Ted Cruz Posts Pics of Himself Delivering Water to Texans
Ted Cruz may have come up with a bright idea on his flight back from Cancun -- if no one else gives him props, he'll do it himself.
www.tmz.com

See this is why we are never going to get rid of this virusUK records 9,834 more Covid cases - down 10% on last week
Covid-19 infection rates have continued to drop with 9,834 more coronavirus cases - a fall of 10 per cent on last week - while the 215 new daily deaths brought Britain's total up to 120,580.www.dailymail.co.uk
Crowds flock to parks and beauty spots on hottest day of the year
Crowds of people broke lockdown rules and flocked to tourist spots across the UK yesterday as they enjoyed sunning themselves during the hottest day of 2021 so far as temperatures hit 60F.

COVID-19: Vancouver man accused of hosting illegal penthouse party faces new charge - BC | Globalnews.ca
Police handed out more than $17,000 in fines and said the suite appeared to be operating as a nightclub and show lounge complete with a stripper pole.
globalnews.ca
Director of care home with worst COVID-19 death toll in B.C. resigns
Vancouver Coastal Health says in a statement that Little Mountain Place recently notified the health authority that its administrator had submitted her resignation.
bc.ctvnews.ca
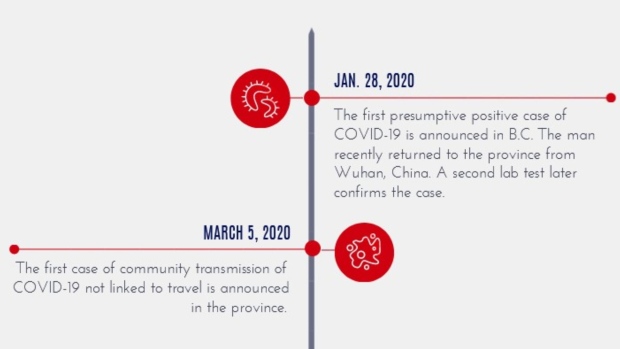
Scroll through this timeline of the 1st year of COVID-19 in B.C.
One year ago, health officials in B.C. announced the first COVID-19 case in the province.
bc.ctvnews.ca
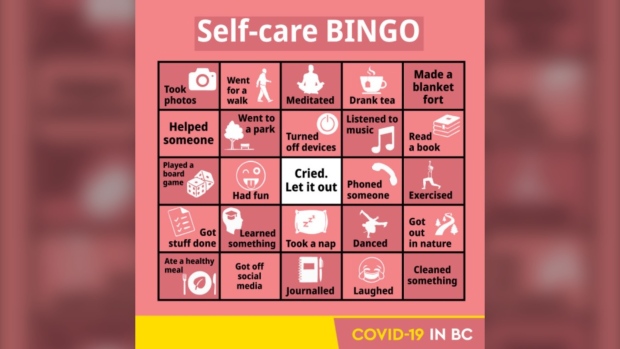
Government Twitter account 'missed the mark' with COVID-19 'self-care bingo' card
The bingo card, which includes a variety of COVID-19 self-care ideas to help manage some stress and anxiety” was shared on the account on Feb. 19.
bc.ctvnews.ca

Isolation and sanitation during COVID-19 may affect human microbiome, scientists say
While it's important to follow public health orders to reduce spread of COVID-19, experts say that all the antibacterial wipes and physical distancing could have long-term impacts on our microbiomes -- the collection of microbes that live on and inside our bodies.
U.K. variant detected at three Surrey schools with COVID-19 exposures
Three recent COVID-19 exposures in Surrey schools have been confirmed to involve one of the variants of concern that health officials around the world have been monitoring.
bc.ctvnews.ca
See this is why we are never going to get rid of this virus
Ain't no getting rid of. That shit is permanent now.